
Stefan  Kertesz, MD@StefanKertesz
Kertesz, MD@StefanKertesz
Kertesz, MDSep 19, 2022
21 tweets
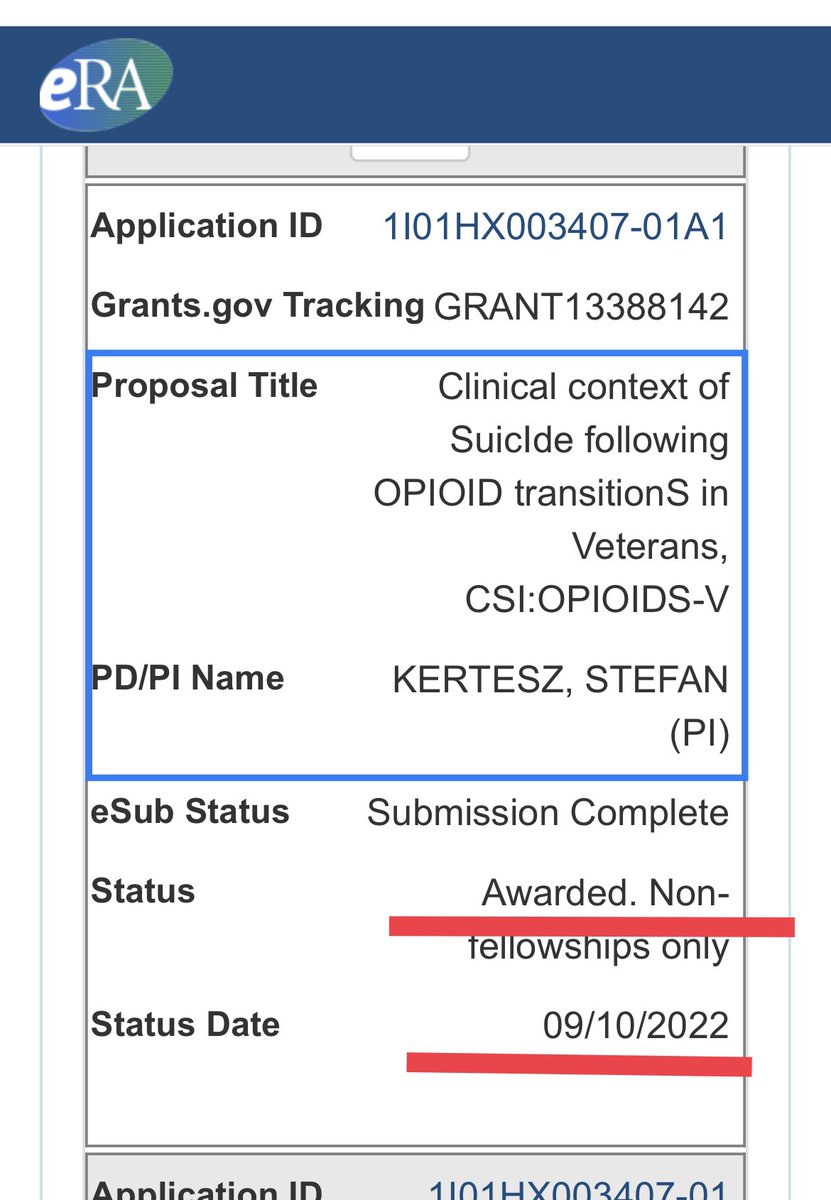
1/Our study to examine suicides after Rx opioid reduction has been FUNDED
It’s called CSI:OPIOIDs-V
We’ll look at suicides in Veterans & non-Veterans
Our outcome target is to help clinicians & healthcare organizations act to prevent these deaths
2/We are compelled to study these suicides because
(a) they’re alarming, and
(b) they occur as part of health care changes justified as being “for safety”
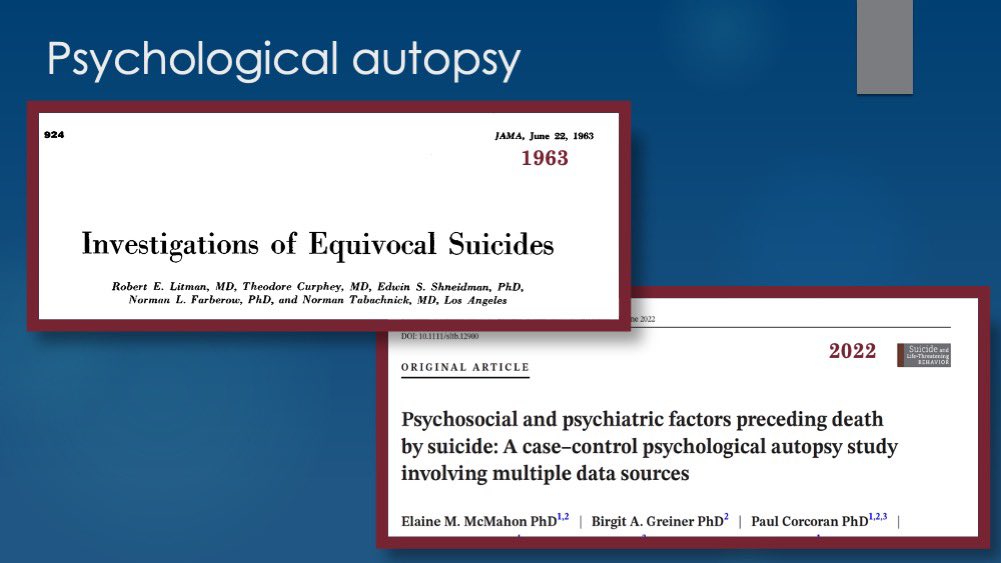
3/Our team of suicide, opioid & pain scholars chose a unique approach for this study  :psychological autopsy.
I wish to explain why
:psychological autopsy.
I wish to explain why
:psychological autopsy.
I wish to explain why 
4/Most studies of Rx opioid  apply stats
to calculate a “net” effect, as if the effects are *uniform*!
apply stats
to calculate a “net” effect, as if the effects are *uniform*!  We know the the “net” effect is often “harm”
But most of what explains why there are BAD outcomes, vs GOOD ones, is *unknown* - which we detail in @JAMA Network Open
We know the the “net” effect is often “harm”
But most of what explains why there are BAD outcomes, vs GOOD ones, is *unknown* - which we detail in @JAMA Network Open
apply stats
to calculate a “net” effect, as if the effects are *uniform*!
We know the the “net” effect is often “harm”
But most of what explains why there are BAD outcomes, vs GOOD ones, is *unknown* - which we detail in @JAMA Network Open 5/The limitations to big database studies are clear:
 By design, they factor OUT most differences between patients, and their life contexts, as *nuisance variables*
Even if researchers wanted to look at these key factors, the retrospective databases don’t reveal them
By design, they factor OUT most differences between patients, and their life contexts, as *nuisance variables*
Even if researchers wanted to look at these key factors, the retrospective databases don’t reveal them
By design, they factor OUT most differences between patients, and their life contexts, as *nuisance variables*
Even if researchers wanted to look at these key factors, the retrospective databases don’t reveal them6/To illustrate the *special* importance of looking at individual suicides, consider a comparison from a different domain:
airplane crashes.
In this video, I focus on the explosion of TWA Flight 800 in 1996
7/If we apply today’s opioid research methods to airplane crashes, we’d:
make a database comparing that stayed up to that crashed, based on standard data for all
We would NOT look at facts unique to crashes (“black boxes”) because they’re not available for alls
crashes, we’d:
make a database comparing that stayed up to that crashed, based on standard data for all
We would NOT look at facts unique to crashes (“black boxes”) because they’re not available for alls
crashes, we’d:
make a database comparing that stayed up to that crashed, based on standard data for all
We would NOT look at facts unique to crashes (“black boxes”) because they’re not available for alls 8/But in the USA, when an crashes, investigators collect *every fact that can be gotten* about THAT crash.
With TWA800, that led to safety recommendations
crashes, investigators collect *every fact that can be gotten* about THAT crash.
With TWA800, that led to safety recommendations9/In the context of SUICIDE, by analogy, that kind of investigation is called “psychological autopsy”
that combines interview & record review. It has been used since 1963
10/Here are *some* of the MANY questions we can get at with psychological autopsy
“How many shared concerns with family & friends?”
“Was there an impasse in clinical care?”
More in the pic
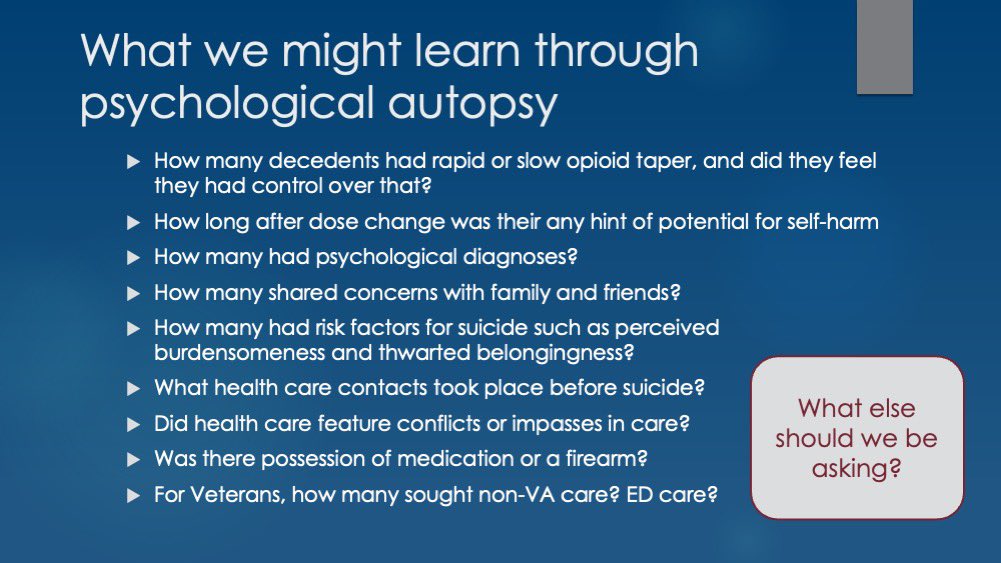
11/What other questions do YOU think we should ask?
12/ This work could protect future patients!
But there are challenges to the work:
Ethical research requires voluntary recruitment of bereaved survivors
There’s no public registry or database we can pull from
So we must *solicit the public*

13/ We have to do our best addressing distrust between survivors and both:
a) Healthcare
b) Researchers
We know researchers can be exploitative, not protective
14/ Transparency is essential.
We’ve been transparent since our pilot study in 2020.
Our detailed briefing is available on Youtube.
youtu.be/a8-GIE65UXQ
15/So how will CSI:OPIOIDS-V work?
Many steps, simplified:
Outreach
A screening survey for people considering our study:
go.uab.edu/csiopioids
A more detailed survey, an interview, and a medical record review with a subset
Together, that’s psychological autopsy
Outreach
A screening survey for people considering our study:
go.uab.edu/csiopioids
A more detailed survey, an interview, and a medical record review with a subset
Together, that’s psychological autopsy 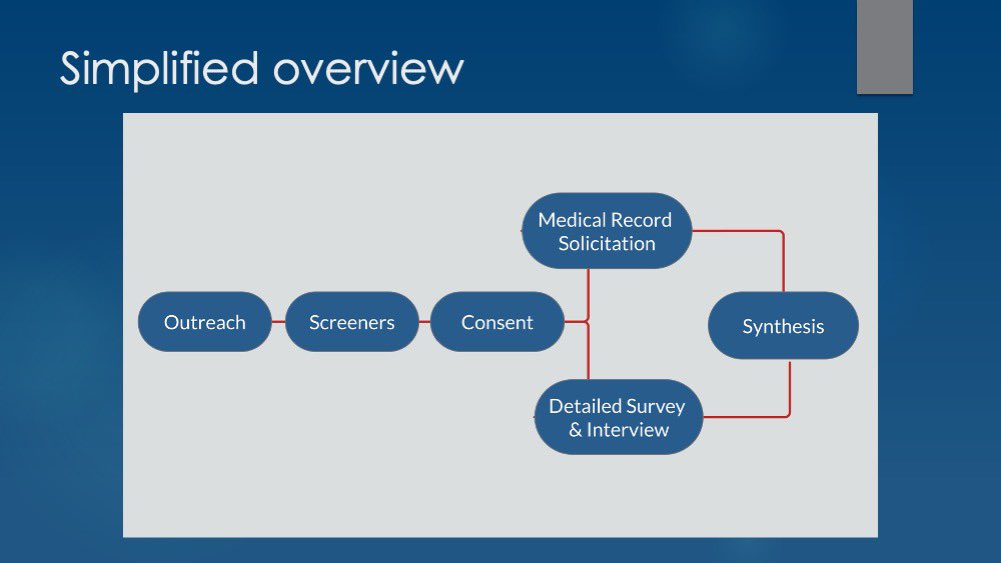
16/We’ll report what we learn, as we learn it.
Many, like @National Pain Advocacy Center & health care leaders are advisors
Together we WILL make recommendations
We’ll submit our work to stringent peer review: we will NOT hide our findings
We will maintain the strictest ethical standards.
17/ If you know someone:
A person who is a family member or CLOSE friend who lost someone to what might have been a suicide after prescription opioid reduction,
Let them KNOW about us.
go.uab.edu/csiopioids
18/If you know an organization that has reach to bereaved survivors, let them know about us too! Reach out to them, and reach out to me in DM.
19/Our first major grant funding is from the Health Services Research & Development branch of the US Department of Veterans Affairs, and we received pilot funding from
Krulak Marine Alliance of Alabama and Department of Medicine at @UAB. We thank all of them.
20/We are proud to partner, as well, with the Tragedy Assistance Program for Survivors @TAPS
This is a leading nonprofit that cares for the families of America’s fallen heroes
taps.org

21/We offer special thanks to the patients & families who told us how much this means to them.
& to:
April Hoge @Adam J. Gordon 🇺🇦🇺🇦🇺🇦 @UAB CAPPI @Allyson Varley @Megan McCullough @Anne Fuqua 🇺🇦 @National Pain Advocacy Center @Caitlin Wolford-Clevenger, Ph.D. @UAB Thomas Joiner, Yogesh Dwivedi, @Beth Darnall, PhD @VA HSR&D

Stefan Kertesz, MD
Kertesz, MD@StefanKertesz
Physician/research in primary care, homelessness, addictions. Professor, UAB. Podcast: @OnHealer he/his https://t.co/cSIpkjx7jD Opinions=mine
Missing some tweets in this thread? Or failed to load images or videos? You can try to .