
Lazarus Long@LazarusLong13
May 30, 2023
20 tweets
A  on near field ( < 6 feet) and far field (>6 feet) aerosols. (To be perfectly frank, this one's for me, but you are invited along the ride into my noggin).
Both airborne, and both important.
Let's start with tweets from aerosol and IAQ scientists.
on near field ( < 6 feet) and far field (>6 feet) aerosols. (To be perfectly frank, this one's for me, but you are invited along the ride into my noggin).
Both airborne, and both important.
Let's start with tweets from aerosol and IAQ scientists.
on near field ( < 6 feet) and far field (>6 feet) aerosols. (To be perfectly frank, this one's for me, but you are invited along the ride into my noggin).
Both airborne, and both important.
Let's start with tweets from aerosol and IAQ scientists.Do aerosols even matter?
Yes. Millions of infectious aerosols emitted per hour in this Dr. Mowaska (technically Ma et Al) study:
academic.oup.com/cid/article/72

The variants are evolving to be better at transmission.
Here we find Alpha to have 18-fold more fine aerosols shed than previous.
academic.oup.com/cid/article/75

Delta and Omicron also evolved to be more transmissible via greater viral load.
Putting that together? Will Covid mutate to become less transmissible? Not likely.
Will actual droplets, not aerosols become more relevant? Not likely.
academic.oup.com/cid/article/76

So, aerosols are important, and getting more so.
Let's dive in.
From 2017, so avoids the accusations of the antimask brigade of pandemic corruption.
twitter.com/linseymarr/sta

Linsey Marr@linseymarr
Jun 28 17
View on Twitter
Relevant for infectious disease transmission: near-source aerosol transmission is more likely rather than assumption of well-mixed room twitter.com/MarshallJulian
"Aerosol concentration decreases w/ distance in "near field."
1.5 m better than 1
2 m better than 1.5"
twitter.com/jljcolorado/st

Prof. Jose-Luis Jimenez@jljcolorado
Sep 24 20
View on Twitter
A4(2). Aerosol concentration decreases w/ distance in "near field."
1.5 m better than 1
2 m better than 1.5
At some point, the problem is the shared air in the room. You are away from directly exhaled "smoke", it is smoke accumulation in room that's risky
#LeapsChat @leaps_org

A two for one here with Dr. Corsi and Dr. Milton - near field is important.
twitter.com/CorsIAQ/status

Richard Corsi, PhD, PE (Texas)@CorsIAQ
Nov 27 20
View on Twitter
1/ I agree with @Don Milton @Don_Milton@med-mastodon.com. It is important to distinguish between near- and far-field aerosol particles. In the near field (close contact) there is potential for much higher concentration of aerosol particles in the breathing zone of a receptor.
A 5 minute near field dose is equivalent to a 35 to 50 minute dose.
twitter.com/CorsIAQ/status
Richard Corsi, PhD, PE (Texas)@CorsIAQ
Nov 27 20
View on Twitter
8/ For these SPECIFIC CONDITIONS (caveat) a 5 min near-field dose is equivalent to a 35 - 50 min far-field dose, certainly realistic exposure times in each. Seems entirely plausible that inhalation dose of virus-laden aerosol particles in near- and far-fields are BOTH important.
Similar line of thinking here in "The Breathmint Study", by @Hooman Parhizkar (my apologies, I tried to resist).
Where breathmint were used methodically as tracers to find that the 20 minute mark was when those tracers blended in.
scholar.google.com/scholar?start=

Respirators help with source control (so it never becomes airborne), and reduction of near field and far field.
Air cleaners help with reduction of near and far field aerosols.
WAIT, WHAT?
Yes.
twitter.com/HuffmanLabDU/s

Alex Huffman, Ph.D. - @ProfHuffman@mstdn.social@HuffmanLabDU
Nov 01 21
View on Twitter
For an inhalable virus, distance matters. Guidance has been:
 Near: concentrated plume; use mask, back away
Far: aerosol builds up; mask, ventilation, filtration
Work by Yugo Li et al. suggests ventilation helps more than expected, even in near-field
onlinelibrary.wiley.com/doi/full/10.11
Near: concentrated plume; use mask, back away
Far: aerosol builds up; mask, ventilation, filtration
Work by Yugo Li et al. suggests ventilation helps more than expected, even in near-field
onlinelibrary.wiley.com/doi/full/10.11
Near: concentrated plume; use mask, back away
Far: aerosol builds up; mask, ventilation, filtration
Work by Yugo Li et al. suggests ventilation helps more than expected, even in near-field
onlinelibrary.wiley.com/doi/full/10.11 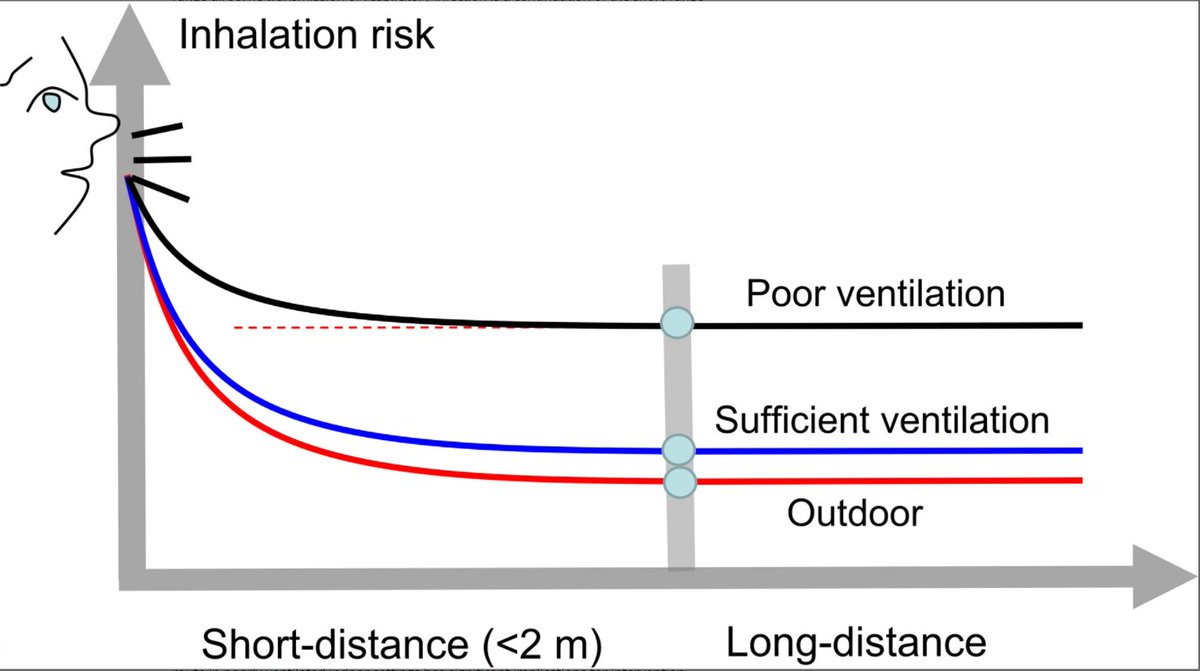
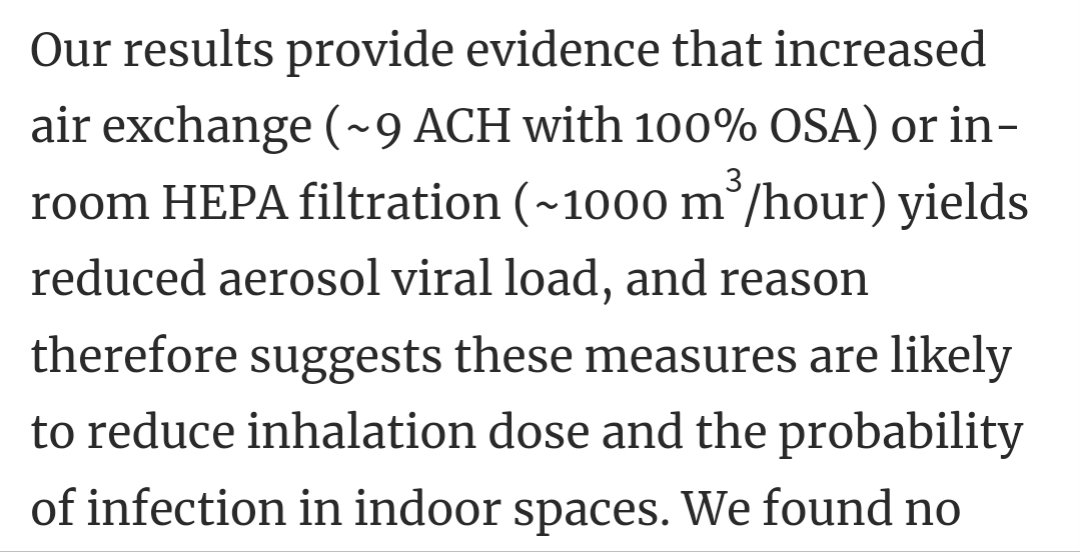
Confirmed in another very interesting study by @Hooman Parhizkar, with 11 participants infected with Covid.
They found that aerosol viral load was reduced with greater ACH. Significantly so, in the case of near field.
But, it reduces for far field, too.
academic.oup.com/cid/article/75

Normally, I try to shy away from models. But Dr. Miller is an exception.
Both near field and far field must be mitigated simultaneously.
Because of the additive nature of both. Think about it.
You, mouth breathing while staring at a brownie for 1
twitter.com/ShellyMBoulder


Shelly Miller, PhD@ShellyMBoulder
Sep 13 21
View on Twitter
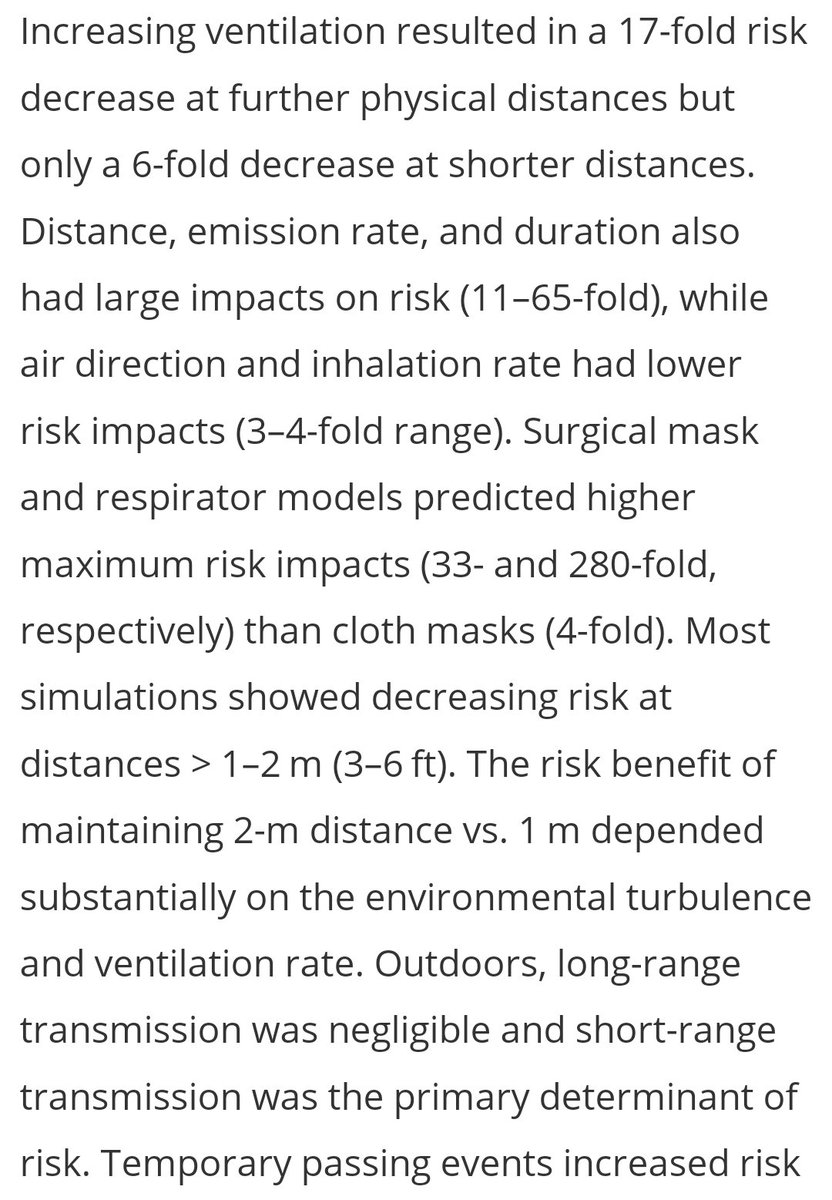
Check out our great new paper led by Dr. Wagner: Modeling the impacts of physical distancing and other exposure determinants on aerosol transmission. Glad to be a part of this analysis, with amazing colleagues Drs. Sparks, Chen, Waldman and Dr. Macher oeh.tandfonline.com/doi/full/10.10

hour.
After 20 minutes, your mouth breath blends in and fills the room (not exact process, for narrative value, please, good Doctors).
But you STILL continue to mouth breathe, and so the concentration of aerosols will still be thickest near you.
What to do?
You reduce risk 17 fold by cleaning the air if far away.
And reduce risk by wearing a respirator by 280 fold.
(Or, if feeling wild, by wearing a surgical mask to reduce risk 33 fold.)
Surgical masks. Yes, respirators are clearly better. But something is better than nothing.
And for source control? In actual measurements of actual viruses, surgical masks did well.
twitter.com/Don_Milton/sta

Don Milton @Don_Milton@med-mastodon.com@Don_Milton
Feb 04 21
View on Twitter
Actual measurement of virus aerosols with and without surgical masks show that they significantly reduce the amount of virus released into the air. doi.org/10.1038/s41591

Another surgical mask source control study.
Are they perfect? No.
Better than nothing? Yes.
Would I wear one? Lol.
twitter.com/linseymarr/sta
Linsey Marr@linseymarr
Jun 14 21
View on Twitter
Surgical masks aren't too terrible for source control. "The overall mask efficiency [including leakage]...is reduced compared to the through-mask filtration efficiency, from 93 to 70% for talking, but from only 94–90% for coughing." nature.com/articles/s4159 by @chris cappa
Finally, vaccinations are important, too.
Because they reduce viral load? From various studies, no.
"Vaccination shortens the duration of time of high transmission potential, minimizes symptom duration, and may restrict tissue dissemination."
academic.oup.com/ofid/article/9
Minimizes duration time of high transmission potential - includes the presymptomatic time.
Minimizes symptom duration. The coughing, sneezing, bathroom, eye gunk.
So, get vaccinated, clean the air, #RespiratorUp - and no butterfly kisses.
Two tweets above, I stated that vaccines do NOT reduce viral load.
I was wrong. Just didn't hit the right studies.
But I just stumbled across this detailed treasure trove of all the ways vaccine reduce those aerosols!
icemsg.org/myths/myth-vac
Viral load reduction.
Reduced duration of infectious period.
Symptoms reduction (like coughing,
etc.
So vaccines will reduce respiratory aerosols, as well.
Back up link
archive.is/pDMRI 



Lazarus Long
@LazarusLong13
Temporarily in Baja California, Mexico with limited connectivity. Former bluecheck.
#CoVidIsAirborne #Masks4All #PZC.
Missing some tweets in this thread? Or failed to load images or videos? You can try to .